
Back to Blog
Care Integration
Prioritization: when demand is great, and resources are limited
By relying on traditional strategies healthcare systems will not be able to address the current demand. Why? Because there is a foundational shift leading the way: designed to deal with acute conditions, they must deal with an always growing number of chronic patients, who require a long-term relationship.

Matilde Ferreira
April 11, 2023 · 10 min read

Long-lasting waiting lists for elective surgery, lengthy waiting lists for medical appointments and endless waiting times for medical care at the emergency room. The reality is well-known by worldwide healthcare systems:
- In England, there are around 40.000 people1 waiting more than 18 months (about 1 and a half years) for surgery, while, last December more than 54,500 patients2 waited over 12 hours in the emergency department to be admitted.
- In Spain, nearly 800,000 people3 are on the waiting list for operations, setting a new record high for having to wait for surgical care and around 20% of patients have to wait more than 6 months, while those that need to be seen by a specialist must wait 79 days.4
- In Portugal, the number of appointments and surgeries performed grew during the last year - 8% and 15%, respectively - but it was not enough to keep up with the demand – that increased 20%.5
And we could keep listing.
It is agreed that people have never demanded so much from the health sector and if nothing changes, those figures will keep spreading in the upcoming times with much more pressure ahead: an expected always growing demand contrasting with the health workers shortage are fostering the perfect storm for healthcare systems.
Putting it plain, approximately one out of three adults suffer from multiple chronic conditions often requiring multiple interactions with different providers.6 On the other hand, the available human resources will be lacking - according to the World Health Organization, there will be a shortfall of 10 million healthcare workers by 2030.7
A global call for change
Traditional and volume-based strategies (in which higher demand is addressed with more resources) are no longer enough, because there is a foundational shift pressing health systems: those systems were originally designed to deal with acute conditions, but today they must deal with an always growing number of chronic patients, who require a long-term relationship with the healthcare system.
We are talking about rethinking and redefining healthcare processes to make them more integrated, more efficient, and more responsive to today’s needs. More than broken services, healthcare systems need to deliver solutions.
The first takeaway that we would kindly ask you to keep in mind is that episodic care, planned based on steady timeframes, careless with the dynamic and unpredictable nature of clinical evolution is not adequate to meet the current needs. Why? Because acute exacerbations of Ambulatory Care Sensitive Conditions don't happen at a set date and time.
So, providers need to promptly address acute needs when they happen, or even better, anticipate them, especially because evidence shows us that around 25% of acute hospital admissions, could be avoided with timely interventions.8 Which means that resources – human, financial and physical - are being used sub-optimally.
Allocative efficiency: the ability to do more with the same resources
The core of this subject can be briefly explained as the ability to allocate the right resources to the right patient at the right time, by improving allocative efficiency.
“Allocative efficiency is about whether to do something, or how much of it to do, rather than how to do it. Allocative efficiency in health care is achieved when it is not possible to increase the overall benefits produced by the health system by reallocating resources (…).” 9
In a scenario in which health systems must keep up with an exponential growing demand while keeping the same human resources – because they won’t be following the same rising trend - allocative efficiency arises as an essential ability to:
- Avoid the waste of resources - understood both as technical resources, appointments’ slots, and healthcare professionals’ time - with stable patients.
- Avoid decompensation and reduce unnecessary hospitalizations or admissions in the Emergency Departments, reducing high-cost healthcare.
Following this line of reasoning, allocative efficiency includes prioritizing patient care, by deciding which patients should be seen, and whom should be seen first, when demand is great, and resources are limited.
Note: this is not about leaving patients unattended or lost on their own, it’s about adjusting the healthcare system answers to each patient, according to his/her risk, taking advantage of the health technologies already in place.
Prioritization: a word to keep top of mind
Patient prioritization, defined as “the process of ranking referrals in a certain order based on criteria”,10 is one of the possible strategies to improve fairness in waiting list management. This practice differs from a first-in first-out (FIFO) approach that ranks patients on waiting lists chronologically, from triage methods used in emergency departments where patients are sorted into broader categories (e.g. low/moderate/high priority or service/no service). Prioritization is related to non-urgent services involving a broader range of timeframes and patient types.10
UpHill approach: prioritization enabled by continuous and automatic monitoring on top of patient-centered care journeys
Care continuity is an unequivocal necessity for today's health systems, creating opportunities for transforming people’s experience of care from disjointed to coordinated, reactive to proactive, and service-orientated to personalized.
Previously, we have explored the essential requirements to connect all the scattered dots of healthcare systems. Long-short story: care journeys are the cornerstone to design a whole new system, without the weight of capital infrastructure, people-tied traditions, and data privacy and security out-of-proportion brakes.
A multidisciplinary and comprehensive care journey works like a map that indicates the path that the patient will follow from the moment he or she is diagnosed, guiding care provision across different healthcare professionals, teams, departments, providers, and care levels. This is the guarantee that each patient receives the appropriate care at each point in time, regardless of where they are, precisely because all the stages the patients must go through and what happens at each stage were previously defined.
The UpHill Care Journey is a stepwise multidisciplinary care plan guiding patient progression through a sequence of milestones translated from guidelines or evidence into personalized contexts, allowing decision support and digital automation of clinical activities, and aiming to standardize care and improve patient’s outcomes and experience.
What does it have to do with prioritization? Everything.
At UpHill, we think on patient prioritization for chronic diseases based on 3 connected dimensions that work on top of care journeys:
- Follow-up: the first step to improve care continuity is continuous patient progress monitoring, and to do so UpHill implements automatic follow-ups using an omnichannel approach with automatic identification of red flags, to conveniently detect patient deterioration ahead of time. This channel works bidirectionally, meaning it also gives the patient the autonomy to report disease deterioration.
- Risk stratification: the second step is about giving an actionable meaning to the data collected. Based on patients’ answers to validated questionnaires and scores, UpHill identifies the patient risk and generates different levels of alerts that warn health teams about the top priority cases.
- Care plan adjustment: finally, based on the risk, the next best actions are suggested (or even automated when applicable), meaning that the care journey is adjusted to patients’ needs. All in all, each step of the care journey is based on the best scientific evidence available, and is flexibly, quickly, and automatically adjusted according to the patient's progress and needs.
The example of two patients with chronic migraine
As it is: currently, in most hospitals, two patients diagnosed with similar severity chronic migraine are followed-up in a sequential rational, based on steady timeframes that does not adapt to the progression of the disease, and for which little to no guidance is found on guidelines and evidence.
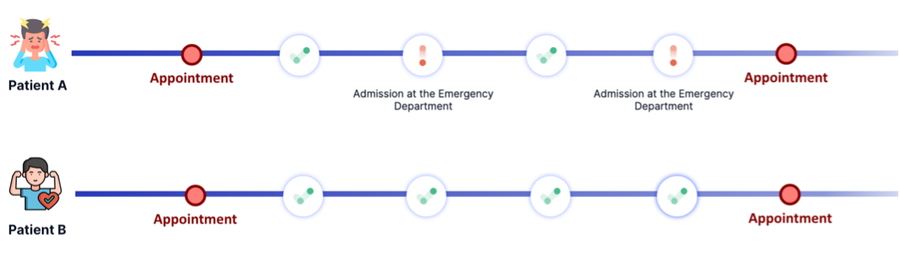
Meaning that two patients being followed by the same clinical team wait exactly the same time to be seen by their doctor again, even considering that:
- Patient A may have two acute episodes between follow-up appointments and may be admitted to the emergency room in both.
- Patient B may have no acute episodes between follow-up appointments.
Additionally, there is an information gap about the disease impact, symptoms evolution, etc., between appointments. In other words, by the time they arrive at their next appointment, patients may be stable (and the appointment is unnecessary) or have already experienced acute episodes that warranted their anticipation. Meaning, we usually use evolution-blind follow-ups.
As to be: with a prioritization care approach, the patient's journey is much more adaptative to patient needs, that can be both reported by the patient or identified by the clinical team. Follow-up mechanisms are triggered to assess the frequency, severity, and duration of crisis episodes and, when necessary, in-person appointments are brought forward.
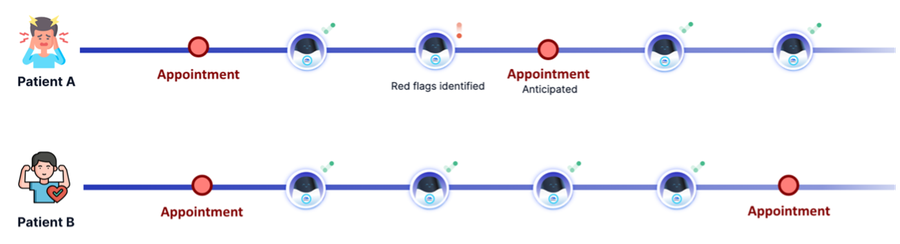
Just like in the previous scenario, these two patients have the same type of migraine, but quite different clinical evolution, requiring different approaches:
- The red flags reported by Patient A are promptly monitored by his/her clinical team, remotely, and the follow-up appointment is brought forward whenever red flags demand for it.
- Without red-flags or additional unforeseen patient need, the schedule follow-up visit is kept.
Key advantages
For patients:
- Better disease management and more convenient care.
- Fast track to healthcare services upon clinical deterioration.
- A sense of proximity that care for their specific needs even between healthcare touchpoints.
For healthcare professionals:
- More time available for the most severe patients and less time spent on follow-up tasks.
- Prevention decompensation by promptly addressing patients’ needs.
For healthcare institutions:
- Better allocative efficiency: more capacity to severe patients, by relieving HCPs from low value tasks.
- Less hospitalizations and readmissions, and less costs, we should say it.
Does prioritization work? “Please, show me the numbers.”
A systematic review of patient prioritization tools in non-emergency healthcare services states that “is difficult to assess these findings considering the variance between research settings and the nature of the considered prioritization system, tool, or process used in the studies”.10 However, it points out several studies that conclude that the prioritization process is associated with lower waiting times.
Additionally, feasibility studies show that 70% of follow-up appointments could be managed by telephone or video or did not need to happen at all11 - which indicates a clear room for improvement when it comes to improve allocative efficiency based on patient prioritization – and many others reveal the exorbitant costs of interventions that could be avoided through better risk stratification, care anticipation and patient prioritization.12-14
UpHill implemented a patient-initiated follow-up use case with a Portuguese University Hospital with promising results: 65% of alerts were solved without an in-person visit to the hospital (saving time and resources) and only 22% of patients who triggered the patient-initiated follow-up were referred to the Emergency Department (avoiding unnecessary visits from other patients).
Get in touch to better understand how UpHill can help your hospital improve allocative efficiency and patient prioritization.
References
- NHS. (2023, February 22). NHS cuts elective backlog with longest waiters down a quarter in one month. NHS England. Retrieved April 14, 2023, from https://www.england.nhs.uk/2023/02/nhs-cuts-elective-backlog-with-longest-waiters-down-a-quarter-in-one-month/
- Neville, S. (2023, January 12). Ambulance and A&E Waiting Times hit new high in England. Financial Times. Retrieved April 14, 2023, from https://www.ft.com/content/1eb9c356-3b93-4efd-a7f9-e461e8c3ee69
- Donmez, B. B. (2023, April 4). Waiting lists for surgery in Spain break new record with almost 800,000 in queue. Anadolu Ajansı. Retrieved April 14, 2023, from https://www.aa.com.tr/en/europe/waiting-lists-for-surgery-in-spain-break-new-record-with-almost-800-000-in-queue/2863273
- Feced, C. G. (2023, January 20). Las listas de espera de la sanidad española: Este es el tiempo que tardan en atenderte u operarte en Cada comunidad. Business Insider España. Retrieved April 14, 2023, from https://www.businessinsider.es/listas-espera-sanidad-espanola-comunidades-autonomas-1187000
- Campos, A. (2023, March 15). SNS Nunca Fez Tantas cirurgias, mas listas de espera continuam a crescer, Diz Fernando Araújo. PÚBLICO. Retrieved April 14, 2023, from https://www.publico.pt/2023/03/15/sociedade/noticia/sns-fez-tantas-cirurgias-listas-espera-continuam-crescer-fernando-araujo-2042462
- Hajat, C., & Stein, E. (2018). The global burden of multiple chronic conditions: A narrative review. Preventive medicine reports, 12, 284–293. https://doi.org/10.1016/j.pmedr.2018.10.008
- World Health Organization. (n.d.). Health workforce. World Health Organization. Retrieved April 13, 2023, from https://www.who.int/health-topics/health-workforce
- High impact change model: Reducing preventable admissions. Local Government Association. (2021, May 26). Retrieved April 14, 2023, from https://www.local.gov.uk/publications/high-impact-change-model-reducing-preventable-admissions
- Shiell A, Donaldson C, Mitton C, et alHealth economic evaluationJournal of Epidemiology & Community Health 2002;56:85-88.
- Déry, J., Ruiz, A., Routhier, F. et al. A systematic review of patient prioritization tools in non-emergency healthcare services. Syst Rev 9, 227 (2020). https://doi.org/10.1186/s13643-020-01482-8
- Cullen, S. (n.d.). Using digital follow-up assessments to reduce unnecessary face-to-face appointments. NHS England. Retrieved April 14, 2023, from https://transform.england.nhs.uk/key-tools-and-info/digital-playbooks/cancer-digital-playbook/using-digital-follow-up-assessments-to-reduce-unnecessary-face-to-face-appointments/
- McDermott KW (IBM Watson Health), Jiang HJ (AHRQ). Characteristics and Costs of Potentially Preventable Inpatient Stays, 2017. HCUP Statistical Brief #259. June 2020. Agency for Healthcare Research and Quality, Rockville, MD.www.hcup-us.ahrq.gov/reports/statbriefs/sb259-Potentially-Preventable-Hospitalizations-2017.pdf.
- Rocha, J.V.M., Marques, A.P., Moita, B. et al. Direct and lost productivity costs associated with avoidable hospital admissions. BMC Health Serv Res 20, 210 (2020). https://doi.org/10.1186/s12913-020-5071-4
- Average annual costs per patient for the top 5% of patients are over 20 times higher than all other patients. (2019, October 29). Retrieved February 28, 2023, from https://www.health.org.uk/news-and-comment/charts-and-infographics/high-cost-high-need-patients

Get the latest on UpHill resources.