
Back to Blog
Acute Care
Two strategies to reduce waiting times in the Emergency Department
Long stays in emergency departments are associated with poorer outcomes and worse patient experience. Can patient journeys be redesigned to reduce readmissions and waiting times?

Matilde Ferreira
February 10, 2023 · 5 min read

Hight affluence combined with inefficient processes makes Emergency Departments (ED) absolutely stressful for those who work there and those who need to visit it. Even conceding that not all the root causes leading to long stays can be addressed from or by the ED, in this blog post we present a new way to shape patient flows during emergency admissions to create time and reduce waits.
1. Improve process efficiency to save time and resources
In this first block, we’ll be exploring some interventions that will help your Emergency Department save time and resources.
- Reduce intra-ER times by implementing a Decision Support System (DSS) that reduces the uncertainty of difficult clinical decisions and the need for unnecessary care.
In the United States of America, overall diagnostic accuracy in the emergency department is high, but some patients – around 6% - receive an incorrect diagnosis.1 Some of these patients suffer an adverse event because of the incorrect diagnosis1 – around 2.0% -, and some of these adverse events are serious1 – around 0.3%. This translates to about 1 in 18 patients receiving an incorrect diagnosis, 1 in 50 suffering an adverse event, and 1 in 350 suffering permanent disability or death.
Even if those figures are comparable to those seen in primary care and hospital inpatient care, it is relevant to emphasize that the main causes pointed for ED diagnostic errors are cognitive errors linked to the process of bedside diagnosis, which could be avoided by providing - in the time and space in which clinical decision-making happens - detailed, updated, multidimensional, and reliable information related to a specific disease.
Additionally, the overuse of healthcare services is widely reported and, in the US system, accounts for as much as 30% of all healthcare spending.2 Overuse takes different forms in different specialties. Unnecessary invasive procedures predominate in some, and medications and screening tests in others. In Emergency Departments, overuse of diagnostic testing is the problem. Once again, the implementation of clinical pathways, detailing the actions, decisions, and criteria for the diagnosis, has been shown to reduce resource waste and hospital costs, specially, if clinical pathways are development under a “de-implementing wisely” framework.3
- Reduce excessive waiting times by redesigning a patient journey that promotes resolutive interactions and reduce the number of patients who leave the Emergency Department without being seen due to excessive waiting.
Now that we’ve thought about ways to reduce resource waste and improve diagnostic accuracy, let’s focus on saving time, by redefining intra-ER patient flow.
Usually, it happens in a standardized way covering multiple steps from admission to discharge or hospitalization. Is it absolutely necessary to wait so long in such fragmented moments before having a resolutive interaction with the physician? Long short story: no, it isn’t, as we suggest establishing different flows for emergent and non-emergent patients.
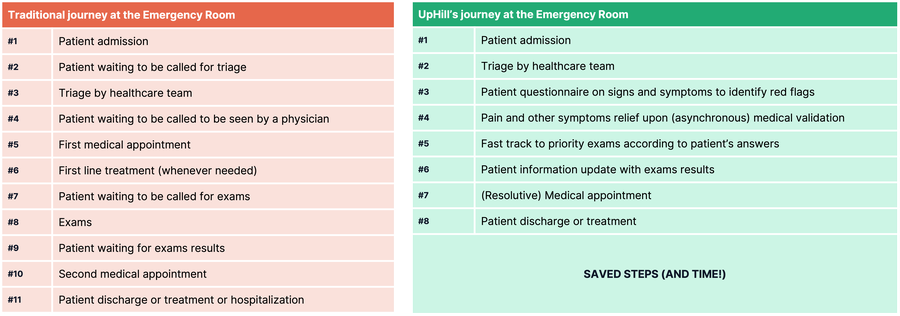
What does it mean?
Physicians will have all the information needed to make accurate decisions the first time they see the patient. Thus, patients will spend less time waiting between interactions and physicians will spend less time in non-resolutive interactions.
Think of Emergency Department navigation as a journey between a fast, convenient, and agile green lane. Now imagine that it is a slow, fragmented, and lengthy path. Which one would you choose?
Put into practice:
- Implement a pathway-based decision support system for differential diagnosis in the emergency room.
- Improve patient stratification using data automatically collected from the patient, using validated questionnaires.
- Anticipate exams to make sure that our teams have the information needed to decide timely.
- Make sure that all software - the one used to collect patients’ data, the decision support system, and the electronic health record - communicate and are automatically updated as new data is available (besides being compliant with legal and regulatory demands)
2. Reduce in-hospitalizations by increasing early discharges safety
Early and accurate identification of patients at low risk of serious illness may improve the flow in the emergency department – as previously described – and by classifying these patients as suitable for discharge. This process represents one of the most vulnerable periods in health care delivery and is described as sometimes being “on the edge”, especially for elderly patients with chronic diseases.
Some challenges remain with discharge effectiveness - ED failure to reconcile medications, patient failure to follow the treatment plan, and patient failure to access post-discharge services are found among the main barriers4 – and can lead to longer-lasting hospitalizations in an attempt to decrease the risk of future readmissions.
On the other hand, evidence found that admission thresholds are higher when the number of emergency inpatients is particularly high, which may indicate that riskier discharge decisions are taken when beds are full.5
To face the aforementioned issues, we suggest two approaches:
- Create and implement a checklist with safety discharge practices to ensure that all critical actions have been completed during admission.
- Implement short follow-up touchpoints to inform patients about results from exams done during admission, therapeutic adjustments, or symptoms evolution.
Put into practice:
- Map and implement a pathway-based decision support system, comprehensive enough to support diagnosis, treatment, and follow-up.
- Create clear decision criteria for discharge and standardize the process.
- Use an omnichannel approach (SMS/Voice/Web) to automate follow-up after discharge.
- Use interoperability capabilities to keep healthcare professionals and patients aware of any relevant update (ex: drug adjustment, readmission, etc)
Final remarks:
Reducing emergency department waiting times requires multiple strategies able to reduce admissions, strengthen referrals for other care settings, improve intra-ER efficiency and reduce discharge risks. In this respect, hospital leaders should strive for having efficient patient flow systems in place, such as streamlined registration processes and well-coordinated transfer of patients between departments, as well as speeding up the process of obtaining patient information and test results, improving communication and collaboration between Emergency Department staff and other healthcare providers.
As umpteen times mentioned, not all the root causes leading to long stays can be addressed from or by the ED, precisely because patient care should not always start and should not finish within the emergency department. The World Health Organization and the OECD have repeatedly pointed out care integration as an unequivocal necessity for today's health systems, creating opportunities for transforming people’s experiences of care from disjointed to coordinated, reactive to proactive, and service-orientated to personalized. There are found hopeful experiences across systems, but some challenges – to explore in future blogposts - remain.
Book a demo to know more about our Acute Care solution.
References
- Newman-Toker DE, Peterson SM, Badihian S, Hassoon A, Nassery N, Parizadeh D, Wilson LM, Jia Y, Omron R, Tharmarajah S, Guerin L, Bastani PB, Fracica EA, Kotwal S, Robinson KA. Diagnostic Errors in the Emergency Department: A Systematic Review. Comparative Effectiveness Review No. 258. (Prepared by the Johns Hopkins University Evidence-based Practice Center under Contract No. 75Q80120D00003.) AHRQ Publication No. 22(23)-EHC043. Rockville, MD: Agency for Healthcare Research and Quality; December 2022. DOI: 10.23970/AHRQEPCCER258.
- Newton E. H. (2017). Addressing overuse in emergency medicine: evidence of a role for greater patient engagement. Clinical and experimental emergency medicine, 4(4), 189–200. https://doi.org/10.15441/ceem.17.233
- Grimshaw, J. M., Patey, A. M., Kirkham, K. R., Hall, A., Dowling, S. K., Rodondi, N., Ellen, M., Kool, T., van Dulmen, S. A., Kerr, E. A., Linklater, S., Levinson, W., & Bhatia, R. S. (2020). De-implementing wisely: developing the evidence base to reduce low-value care. BMJ quality & safety, 29(5), 409–417. https://doi.org/10.1136/bmjqs-2019-010060
- Boonyasai, R.T. et al. (2014) Improving the emergency department discharge process: Environmental ..., Agency for Healthcare Research and Quality. Available at: https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/systems/hospital/edenvironmentalscan/edenvironmentalscan.pdf (Accessed: January 30, 2023).
- Wyatt S, Joshi R, Mortimore JM, et al. Relationship between emergency department and inpatient occupancy and the likelihood of an emergency admission: a retrospective hospital database study Emergency Medicine Journal 2022;39:174-180.






Get the latest on UpHill resources.