
Back to Blog
Biomedical Simulation
Using simulation to maximize clinical pathways implementation
Find out how simulation has a role to play in clinical pathways’ implementation.

Matilde Ferreira
March 30, 2021 · 7 min read
Influenced by the training processes in aviation, high-fidelity simulation kicked in all areas of health sciences, with particular emphasis on medicine and nursing. By the time, it was realized that it was necessary to keep proficiency both in unusual critical situations and usual practices that occur daily. Specialties such as Obstetrics or Anesthesiology 1,2 were at the forefront of its development and application within the sector with the first steps being taken early in the 18th century. However, in the 19th century clinical simulation has become a broadly used technique, moving from Europe to the United States of America. 2
Over the years, the use of simulation has gone from low fidelity to high fidelity models, and in the last two decades there has been an exponential growth in its application in the training of students and health professionals and a strong awareness of this methodology. 3
Simulation: what does scientific evidence show about its impact?
- Reduces asymmetries between theoretical knowledge and care practice. 4-6
- Allows to control a sequence of tasks and prevents risk situations, allows students and professionals to fail in a controlled environment, and confronts each person with its limits. 6
- Supports health organizations’ efforts to promote continuous medical education. 7-9
- Increases the professionals’ degree of confidence in critical moments when the time to make decisions is short and improves ongoing chronic disease management. 7-9
- Positively impacts patients' outcomes. 10
A step inside clinical pathways challenges
As highlighted in past articles, the provision of quality hospital services depends on the suitable and efficient execution of processes. Thus, it’s easy to understand that to improve quality you need to change processes, and consequently human behaviors. However, this doesn't happen twice: most of the healthcare institutions have an oversimplified view of the actual conduct in a patient careflow, based only on outcome measurement. The thing is this approach doesn’t reflect which decisions led to that particular result and so, by widening the time frame, results fluctuate randomly.
The only exception happens when the clinical decision process is structured, and this is all about clinical pathways. Clinical pathways are tools used to translate clinical practice guideline recommendations into clinical processes of care within the unique culture and environment of a healthcare institution. Medical literature points out several advantages of clinical pathways in care quality, units’ efficiency, and patients’ outcomes, but there are remaining barriers to their implementation.
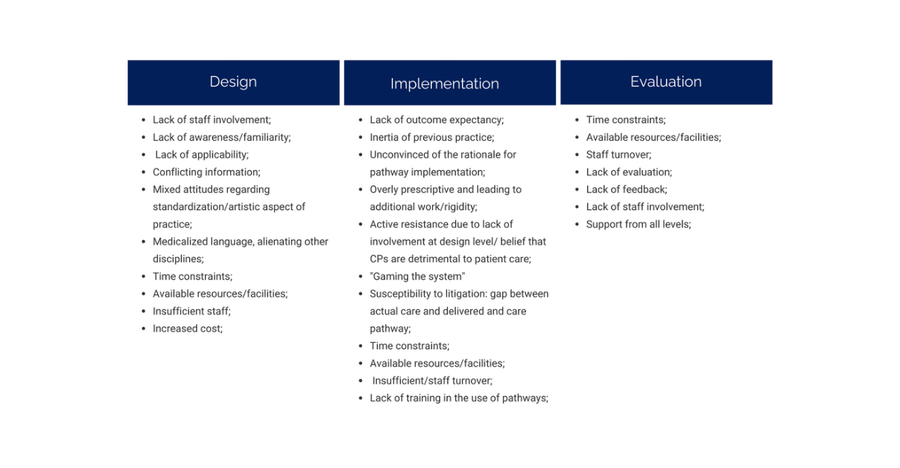
Focusing specifically on barriers that impede clinical engagement and uptake of care pathways, Evans-Lacko, S., Jarrett, M., McCrone, P. et al. gathered the clinician-related factors and distinguished three different levels: 11
Simulation and clinical pathways implementation: a speck of light at the end of the tunnel
Going deeper on this topic, below we recall five quality improvement challenges pointed out by the Healthcare Foundation [12] touching some of the aforementioned issues - namely clinicians inertia and resistance, lack of involvement, applicability, awareness, or outcome expectancy – and explain our vision on how simulation is useful to overcome them.
On a first level, the Health Foundation analysis suggests that in the design and planning of improvement interventions, it is important to establish with the key audiences that there is a real problem to be addressed and why it matters locally; ensure that the evidence-base is of sufficient quality to convince people that the proposed intervention will work, use data collection to track progress and stimulate engagement and learning.
- Convincing people that there is a problem
Authors explain that the literature is full of examples of interventions where clinicians insist that the service being provided is already good. Therefore, those designing and planning an intervention must be careful to target problems that are likely to be accepted as real and that the improvement activity will offer a relative advantage over the status quo.
Solution: when using our clinical simulation software, you are able to give clinicians clear and customized insights on how their actions affect patients' outcomes and which changes would drive better results. - Convincing people that the solution chosen is the right one
According to this report, a second fundamental challenge is to convince people that the right approach to tackling the problem has been selected. Thereby, having a sound scientific evidence base for improvement interventions is likely to be important to the chances of success.
Solution: in addition providing customized feedback on a particular healthcare professional performance, simulation allows each professional to check the scientific evidence supporting the performance assessment, working as a credibility stamp for the solution chosen, which, in this case, represents a clinical pathway designed to work as a roadmap to all teams treating patients with the same conditions. - Getting data collection and monitoring systems right
Data collection is an essential element of the process of improvement. Good quality data are the key both to demonstrating the problem and showing how it is being addressed. Additionally, the research found that some clinicians were reluctant to take part because they had not been consulted in the development of a care bundle.
Solution: our clinical simulation software is useful to collect data at two different points in time: before designing a clinical pathway, in order to have a global perspective on how your staff approaches a particular disease; after designing a clinical pathway to evaluate the new behaviors and its compliance to best practices. Besides, it has an internal feedback system that gives each user the possibility to agree or disagree with a particular recommended action.
Another topic evident from evaluation reports and the literature relates to the profound impact of organizational and institutional context on improvement efforts. This includes organizational cultures, organizational capacity, user involvement, etc. - Organizational cultures, capacities, and contexts
Not surprisingly, organizational cultures supportive of personal and professional development, and committed to improvement as an organizational priority, are more likely to provide an environment where improvement can flourish. However, it’s relevant to clarify the basis reasons of a quality improvement activity since it impacts staff engagement. Literature also reinforces complexity and lack of adequate structures to support improvement activities as a means to failure.
Solution: besides giving quantitative and qualitative insights on your unit performance, more advanced simulation software provides you an intuitive and data-based means of evaluating clinical pathways applicability in the real world, making sure that you’re adding complexity to your staffs’ routine without a clear purpose. Furthermore, this software mimics an electronic health record (EHR), facilitating professionals’ onboarding processes. - Tribalism and lack of staff engagement
In contrast, “resistance to improvement based on ideals of professional autonomy, impermeable boundaries between professional groups, and resistance of professional cultures to change led from outside have all impeded efforts to improve quality”, stated the Health Foundation in a quality improvement challenges report published in 2012. Peer support was highlighted as an important feature in several projects.
Solution: clinical simulation software work also as a training tool, in which health professionals can practice their approach to particular conditions in a safe and predictable environment. Also, it exceeds the personal dimension and ensures process standardization within a healthcare unit, regardless of the experience or expertise level of a particular professional.
Wrap up: in which dimensions can simulation be useful to create a successful clinical pathways strategy?
- To understand the clinical processes in your hospital;
- To test clinical pathways applicability in real world;
- To train clinical pathways, making the teams aware of its recommendations;
- To design future formative programs according to insights extracted;
- To give clear and customized feedback on each performance.
There are many other topics in which we can help you to make evidence-based medicine a reality in your hospital. Have a look at UpHill’s solutions.
References
- [1] Green M, Tariq R, Green P. Improving Patient Safety through Simulation Training in Anesthesiology: Where Are We? Anesthesiol Res Pract. 2016;2016:4237523. doi: 10.1155/2016/4237523. Epub 2016 Feb 1. PMID: 26949389; PMCID: PMC4753320.
- Owen H. Early use of simulation in medical education. Simul Healthc. 2012 Apr;7(2):102-16. doi: 10.1097/SIH.0b013e3182415a91. PMID: 22374231.
- Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach. 2005 Jan;27(1):10-28. doi: 10.1080/01421590500046924. PMID: 16147767.
- Tuttle, N., Horan, S.A. The effect of replacing 1 week of content teaching with an intensive simulation-based learning activity on physiotherapy student clinical placement performance. Adv Simul 4, 14 (2019). https://doi.org/10.1186/s41077-019-0095-8
- Morgan PJ, Cleave-Hogg D, Desousa S, Lam-McCulloch J. Applying theory to practice in undergraduate education using high fidelity simulation. Med Teach. 2006 Feb;28(1): e10-5. doi: 10.1080/01421590600568488. PMID: 16627314.
- Weller JM. Simulation in undergraduate medical education: bridging the gap between theory and practice. Med Educ. 2004 Jan;38(1):32-8. doi: 10.1111/j.1365-2923.2004. 01739.x. PMID: 14962024.
- Toback SL, Fiedor M, Kilpela B, Reis EC. Impact of a pediatric primary care office-based mock code program on physician and staff confidence to perform life-saving skills. Pediatr Emerg Care. 2006 Jun;22(6):415-22. doi: 10.1097/01.pec.0000221342.11626.12. PMID: 16801842.
- O'Connor PJ, Sperl-Hillen JM, Johnson PE, Rush WA, Asche SE, Dutta P, Biltz GR. Simulated physician learning intervention to improve safety and quality of diabetes care: a randomized trial. Diabetes Care. 2009 Apr;32(4):585-90. doi: 10.2337/dc08-0944. Epub 2009 Jan 26. PMID: 19171723; PMCID: PMC2660457.
- Morrow R, Fletcher J, Mulvihill M, Park H. The asthma dialogues: a model of interactive education for skills. J Contin Educ Health Prof. 2007 Winter;27(1):49-58. doi: 10.1002/chp.94. PMID: 17385732.
- Zendejas B, Brydges R, Wang AT, Cook DA. Patient outcomes in simulation-based medical education: a systematic review. Journal of General Internal Medicine. 2013 Aug;28(8):1078-1089. DOI: 10.1007/s11606-012-2264-5.
- Evans-Lacko, S., Jarrett, M., McCrone, P. et al. Facilitators and barriers to implementing clinical care pathways. BMC Health Serv Res 10, 182 (2010). https://doi.org/10.1186/1472-6963-10-182
- Dixon-Woods M, McNicol S, Martin G. Ten challenges in improving quality in healthcare: lessons from the Health Foundation's programme evaluations and relevant literature. BMJ Quality & Safety 2012;21:876-884.

Get the latest on UpHill resources.